Each of our six clinic sites is implementing team-designed quality improvement (QI) projects to improve care for diabetes patients.ÿ QI projects follow the Model for Improvement plan-do-study-act methodology and are supported by experts from the field.

Each clinic has organized a diverse team of quality improvement champions.ÿ Champions represent staff from all areas of the clinic: check-in staff, referral coordinators, medical assistants, providers, and administration.ÿ Teams meet frequently to look at data, plan and implement projects, and track changes over time.ÿ Teams have access to a coach who can help answer questions, provide evidence-based examples and models, and assist with data collection and analysis.
Quarterly, all teams come together in Learning Sessions to share progress, troubleshoot barriers, and provide peer support.ÿ Each meeting has a theme relevant to the stage of implementation or common challenges/opportunities across sites.ÿ The quarterly meetings help to keep everyone on track with their QI goals while providing a sense of camaraderie. They are also helpful to assure that protected time is set aside for teams to plan their next steps.ÿ Each site hosts a meeting on a rotating basis.
 Improvement projects are selected by teams based on perceived need, potential benefit to patients, and feasibility considering competing clinical priorities and organizational culture. ÿHealth center improvement related to diabetes care is assessed every 6 months using an adapted version of the Assessment of Chronic Illness Care survey.
Improvement projects are selected by teams based on perceived need, potential benefit to patients, and feasibility considering competing clinical priorities and organizational culture. ÿHealth center improvement related to diabetes care is assessed every 6 months using an adapted version of the Assessment of Chronic Illness Care survey.

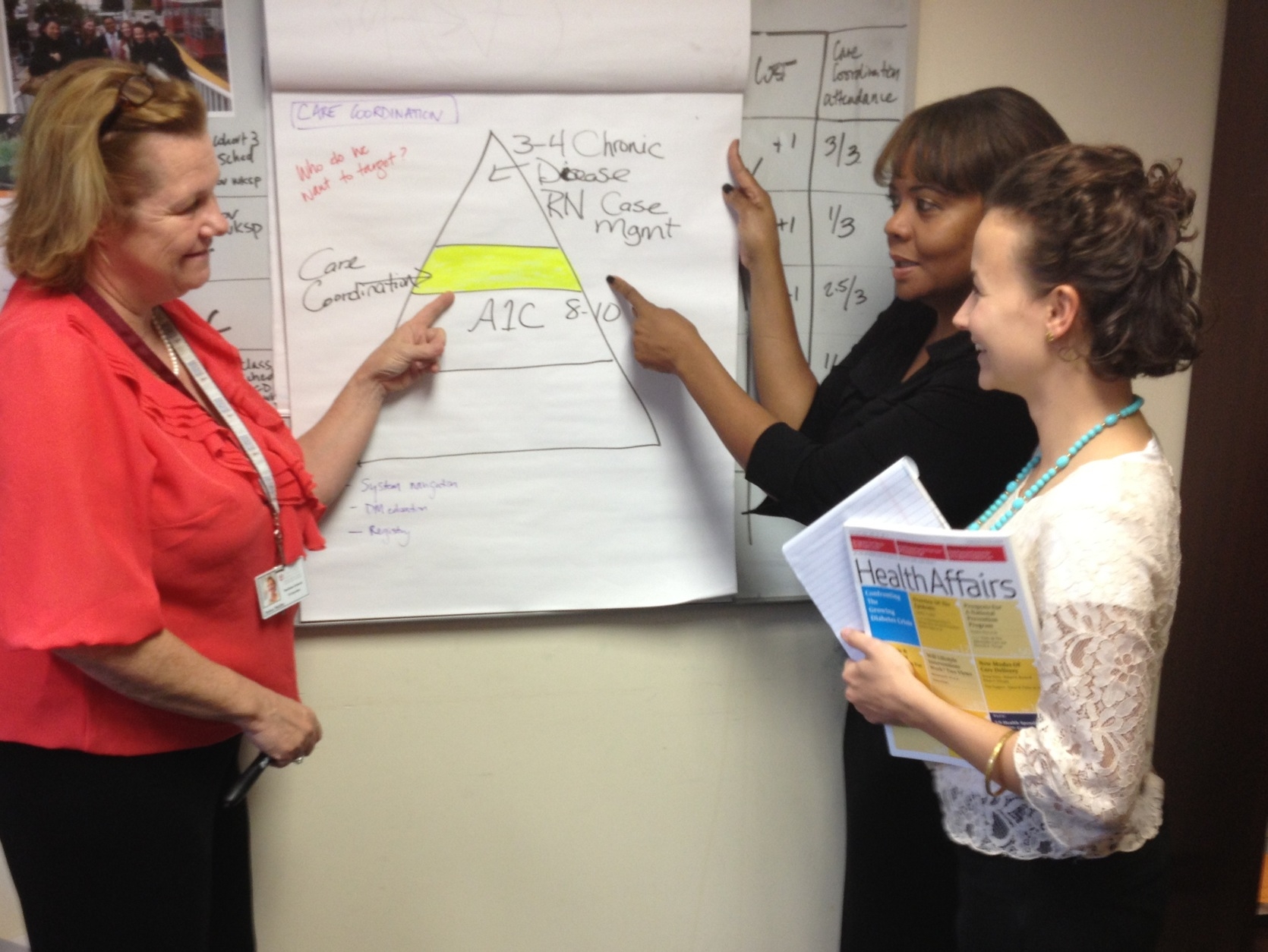
Quality Improvement Projects:
Participating clinics are currently focusing their QI efforts on pilot testing care coordination for small groups of high need patients. This process includes:
- Utilizing diabetes rosters to identify and track high-risk diabetes patients
- Effectively reaching out and engaging patients in their care
- Assessing patient needs and developing a comprehensive care plan reflecting provider and patient goals
- Developing workflows and communication resources to facilitate team based care
- Referral tracking and follow-up
- Referrals to appropriate community based organizations

Past quality improvement projects included:
- Needs assessment to determine patient diabetes self-management barriers
- Medication cards to help patients understand and keep track of the medications they take
- Flowsheets to standardize and improve consistent documentation of diabetes measures
- Appropriate use and tracking of internal referrals to nutritionist and diabetes educators
- Appointment reminder cards to flag patients who need to schedule follow-up visits
- The addition of a diabetes resource room to improve provider access to diabetes materials and to promote referrals to community programs
- Utilization of the Chicago ?Prescription for Fitness? program, run by the Chicago Park Districts (provides free gym membership for up to 6mo for patients with obesity related conditions)
- Phone-based diabetes care management
- ?Diabetes Allstar? group of patients that try out community resources (e.g. exercise programs) and report back to the group
- Diabetes group visits (shared medical appointments)